With the COVID-19 pandemic being prevalent at this time, Montana State Fund (MSF) has released recommendations for clinics who are providing telephonic or virtual services to our injured workers during this crisis:
We thank you for being flexible during this time and if you have any questions, please let us know. We want to thank providers for continuing to see our injured workers in this time of uncertainty and wish everyone safety and wellness! Please see below for approved telemedicine services for MSF:
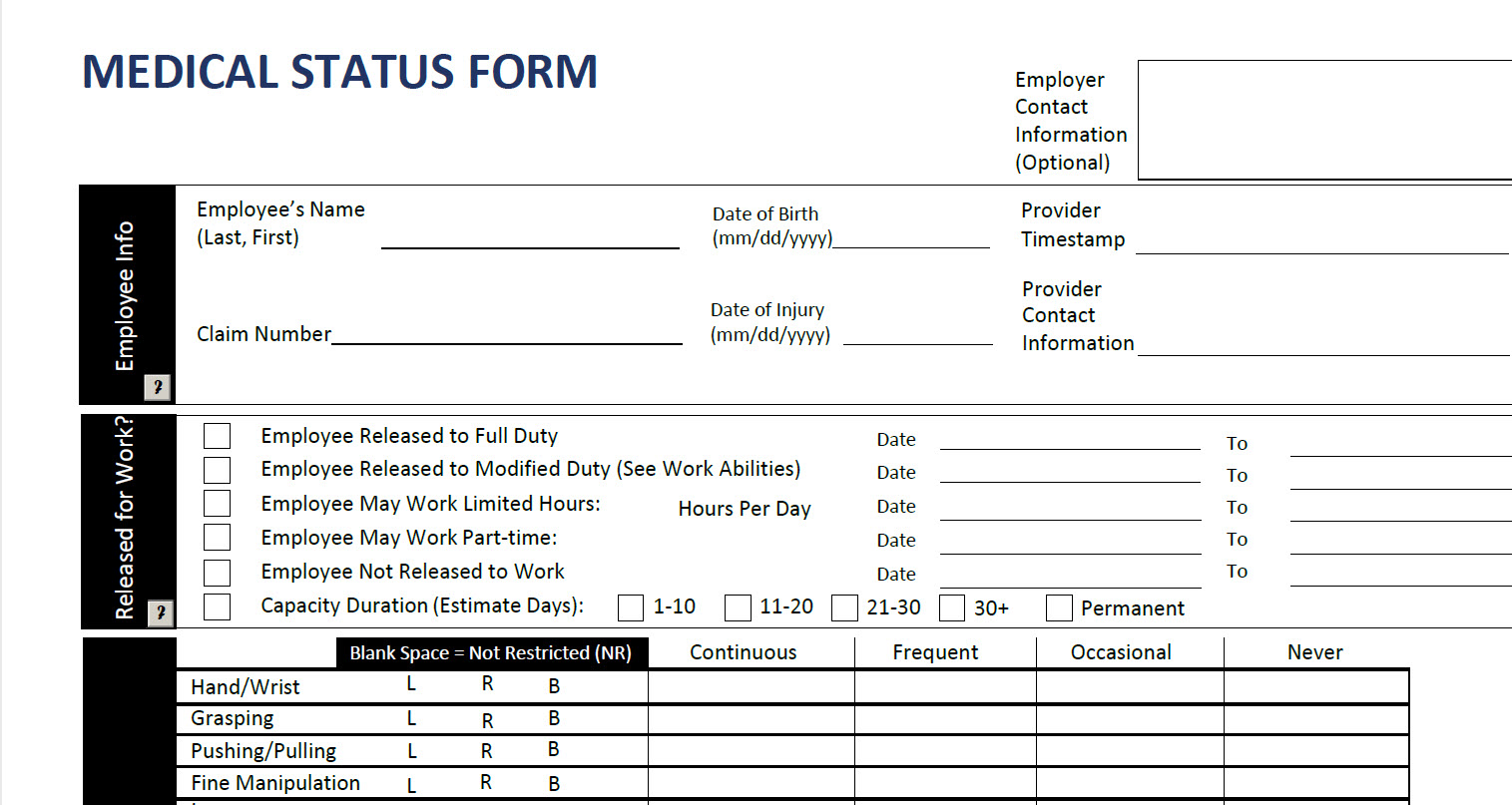
Note: Please use POS 02 in Box 24B of the CMS 1500 form to indicate that the services provided have been via a telephonic/video type method. The GT modifier may also be applied for audio/video telecommunications. For timed codes, please document total time spent in the record.
99201 – 99215 Evaluation and Management visits that normally require face to face time will be allowed as audio/video visits. Documentation does need to support the services billed.
Psychotherapy services
90832: 30 minutes
90834: 45 minutes
90837: 60 minutes
Psychological Evaluations will need to be authorized prior to service by calling Michele Fairclough, Director of Medical Services, at 406-495-5362.
Online Digital Evaluation and Management service, for an established patient, for up to 7 days, cumulative, for up to seven days:
99421: 5-10 minutes
99422: 11-20 minutes
99423: 21 or more minutes
Telephone Evaluation and Management (E/M) services by a physician or other qualified health care professional who may report E/M services provided to an established patient:
99441: 5-10 minutes
99442: 11-20 minutes
99443: 21-30 minutes
Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient or episode of care initiated by an established patient:
98966: 5-10 minutes
98967: 11-20 minutes
98968: 21-30 minutes
Qualified non-physician health care professional online digital (non-face to face) E/M service utilizing internet resources for an established patient, for up to 7 days, cumulative time during those 7 days:
98970: 5-10 minutes98971: 11-20 minutes
98972: 21 or more minutes
Physical/Occupational Therapy can use the above codes as applicable; also, MSF will allow the following re-evaluation codes:
97164 – Physical Therapy Re-evaluation
97168 – Occupational Therapy Re-evaluation
The following Physical or Occupational Therapy initial evaluations will need to be pre-authorized by calling Michele Fairclough at the number listed at the end of this publication:
97161
97162
97163
97165
97166
97167
For physical/occupational therapies, MSF will allow the following codes for a total of 2 units (30 minutes) for the management of home exercise:
97110
97530
97535
We understand that there may be questions regarding different circumstances as we go along. Please call Michele Fairclough, Director of Medical Services, at 406-495-5362 or Kym Vonada at 406-495-5389 and we will work toward getting these issues resolved.
 Report an Injury
Report an Injury Get Coverage
Get Coverage Manage Policy
Manage Policy Pay Bill
Pay Bill